
“I’m doing fine with “shelter in place”,” the 89-year old mom told her physician son, “but I wonder when this will end and what comes next?”
That question is doubtless on everyone’s mind right now. But the answer really depends on how we respond to this public health emergency. As Dr. Harvey Fineberg stressed last week in his article in the New England Journal, if we take the right actions now, we could be relaxing restrictions and going back to work in 10 weeks.
But we have yet to respond to this epidemic the way that Norway, Iceland, China and South Korea have, countries where the epidemic is being or has been relatively quickly and effectively brought under control. I look at their epidemic curves in admiration (you have to click on the logarithmic version to see the flattening of the curve) –they are so impressive: they are smoothing out or falling–a sign of success. Ours is headed straight up–in a very worrisome exponential fashion classic for an uncontrolled epidemic. On Friday, the Infectious Disease Society of America warned that if this trend continues, it could result in many more deaths than predicted.
But it doesn’t have to be that way. Some authors, like Tomas Pueyo, suggest that if we take the right steps now, deaths worldwide could number in the thousands–rather than possibly in the millions. And we don’t have to reinvent the wheel–we can mobilize the basic principles of epidemic containment that the above countries have done so effectively. Those basic pandemic containment principles were successful even without deploying new therapies or vaccines. And if we had followed their lead early on, our numbers could be looking like theirs right now. But it’s not too late — if we act immediately.
This successful multi-pronged effort varied among countries but included:
- A rapid expansion of the healthcare workforce;
- A mitigation, or “social distancing” program far more comprehensive and effective than ours;
- Limiting transmission of infection using dedicated infirmaries;
- Protection of vulnerable populations, in particular the healthcare workforce — with adequate protective equipment and free housing;
- Extensive testing and contact tracing.
A Robust and Protected Workforce
China immediately called into action a vast workforce to bolster overtaxed health care systems: over 40,000 healthcare workers were mobilized from across China to help Wuhan. We have yet to do this in the US, although the need is great: last week, Governor Andrew Cuomo of New York appealed to health professionals across the country to join forces to combat COVID in his state. In China, lack of protective equipment (PPE) led to rapid increases in infections among health care workers initially, followed by a subsequent rapid drop in infections as protective gear was rapidly mobilized; we have yet to mobilize a concerted national effort to remedy the serious PPE shortages in the US.
Comprehensive and Effective Mitigation (Social Distancing)
While all of the countries where coronavirus was brought quickly under control practiced mitigation, also known as social distancing, Dr. Xihong Lin, speaking at the Broad Institute in Cambridge, noted that the program in Wuhan was robust and comprehensive. Wuhan did not just have a “stay at home” order, but a travel/traffic ban and “cordon sanitaire” such as the ones that were implemented in the United States during the 1918 influenza pandemic (it is interesting that a country doctor successfully worked to keep influenza out of Gunnison, Colorado with strategies much more aggressive than anything currently being implemented in the US).
More stringent mitigation strategies used abroad also include limiting how frequently people go grocery shopping — a not insignificant intervention, since every time people go to stores they increase the likelihood of becoming infected. Wuhan provided for home delivery of food. Several of the successful countries are using enforcement measures like issuing fines ($1,500 for breaking quarantine in Norway) and promising jail time for persons who disobey stay at home orders or knowingly spread coronavirus. Norwegians are not allowed to travel to their vacation homes, for fear of overloading the already strained rural health care systems; and they may not travel from one part of the country to another.
Why Mitigation is not Enough
But several epidemic models and the experience in Wuhan suggest that mitigation alone is not enough–that it may leave people on lockdown for months and likely will not stop this epidemic because asymptomatic or mild cases will keep infecting new individuals in our communities. This very clever video offers a visual of why this is so –and why we should be pursuing other strategies to limit transmission in addition to more aggressive distancing.
Limiting transmission
In Wuhan, the most successful strategy to limit transmission involved using isolation infirmaries for infected cases and contacts– just as we did in the United States in the early 1900s when tuberculosis was a significant public health challenge in this country.
According to Dr. Lin, although mitigation slowed the increase in cases in Wuhan, it did not control it. She lists two reasons that mitigation failed: the first was that using the “honor system” of social distancing was not effective since it was difficult to ensure that infected cases did not go out shopping for food and infect others.
Another reason that distancing alone didn’t work is that transmission within families is common: it accounts for 75-85% of COVID clusters. Those family members then go on to infect others in the family and community. For that reason, in Wuhan, hotels and infirmaries were designated for infected and presumptive cases to safely be taken care of apart from their families, so they wouldn’t infect them.
To this end, two new hospitals were set up for the sickest patients and 16 field hospitals were built in converted stadiums for mild cases. Hotels and university dorms that had been left empty due to the “stay at home” order were used for presumptive cases and close contacts, so that they could be followed while in quarantine. If their symptoms worsened, they could be quickly transferred to the infirmaries or hospitals. If patients developed severe symptoms in the field hospital, they were immediately transferred to the dedicated nearby intensive care hospital units.
The end result: fewer new infections, less pressure on hospital systems, and increased ICU capacity.
As part of their strategy to limit transmission, healthcare workers were provided with free housing so they would not infect their families. Interestingly, front line health care workers were found to be the most commonly infected group, and therefore vulnerable.
In Wuhan, these intensive suppressive measures were started on February 2nd. The six hospitals were disassembled on March 10th–approximately five weeks later. And the last case reported in Wuhan was on March 5th. The suppression strategy worked (see table below).
Dr. Fineberg supports using this approach in the United States, saying that we too could end this epidemic in 10 weeks if we employed a similar strategy. In his NEJM article, he recommends that we “Establish infirmaries by utilizing empty convention centers, for example, to care for those with mild or moderate disease and at low risk; an isolation infirmary for all patients will decrease transmission to family members. Convert now-empty hotels into quarantine centers to house those who have been exposed, and separate them from the general population for 2 weeks; this kind of quarantine will remain practical until and unless the epidemic has exploded in a particular city or region.”
This approach is already being implemented in New York City. And some hotel chains in the US are in discussions to broaden this approach across the country: health care workers would be housed in hotels, where they could live safely apart from their families and not infect them, and tents could be constructed in parking lots or nearby stadiums that would be for symptomatic cases. But state and local governments should start to organize now to think about how this approach can be tailored to every community in the country.
Testing and Contact Tracing
In Wuhan, once the epidemic was under control, testing was used across the whole community to find and isolate cases so they could not infect others. Staff surveyed every household. And then they prioritized testing to those with symptoms and their contacts.
The result? Reduced transmission, immediate medical care for those who needed it, and, since mild cases were treated in a timely fashion, fewer cases progressed to severe or critical cases.
In the U.S., this strategy is starting to be set in motion also. Dr. Bill Burman, head of Denver Public Health, posits that testing and contact tracing will be a key strategy to keep the virus in check once the epidemic curve starts to “flatten” and there are fewer cases. The public health department there is starting to implement a “South Korea” strategy in Colorado now: “we in public health and healthcare will need to develop ways to test widely and efficiently,” Dr. Burman said. In Massachusetts, Partners in Health has just been tapped to start a contact tracing and testing program, a welcome intervention since testing and contact tracing of symptomatic cases not requiring hospitalization has been lacking here.
So what would constitute effective next steps? Better mitigation, infirmaries to limit transmission and more screening.
- A substantial increase in a dedicated health professional workforce;
- Continued and more effective distancing, with travel bans and limits on trips to grocery stores and pharmacies, and mechanisms to enforce these;
- Limiting transmission through the widespread use of infirmaries for mild-moderate cases and isolation in hotels and college dorms of case contacts;
- PPE to protect health care workers and dedicated housing for health professionals, so they will not infect their families;
- Extensive testing and contact tracing.
An effective public health response will cut short the brisk upward spiraling of preventable deaths due to cycles of infection and reinfection that we are seeing now. According to Dr. Lin, the experience of other countries shows that the end could be in sight– “if we do it right.”
Table 1.
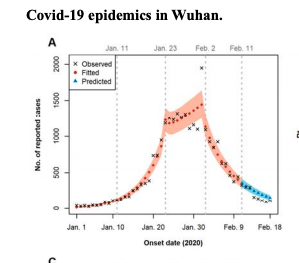
Table from Lin et al showing the initial brisk rate of transmission in Wuhan (transmission rate 3.88) which dropped substantially to 1.36 after mitigation measures (note the slower increase in cases from Jan 23rd to February 2nd); but abruptly dropped (transmission rate, 0.32) after institution of infirmaries on February 3rd.
Photo credit: photo by Tim Foster from Unsplash.